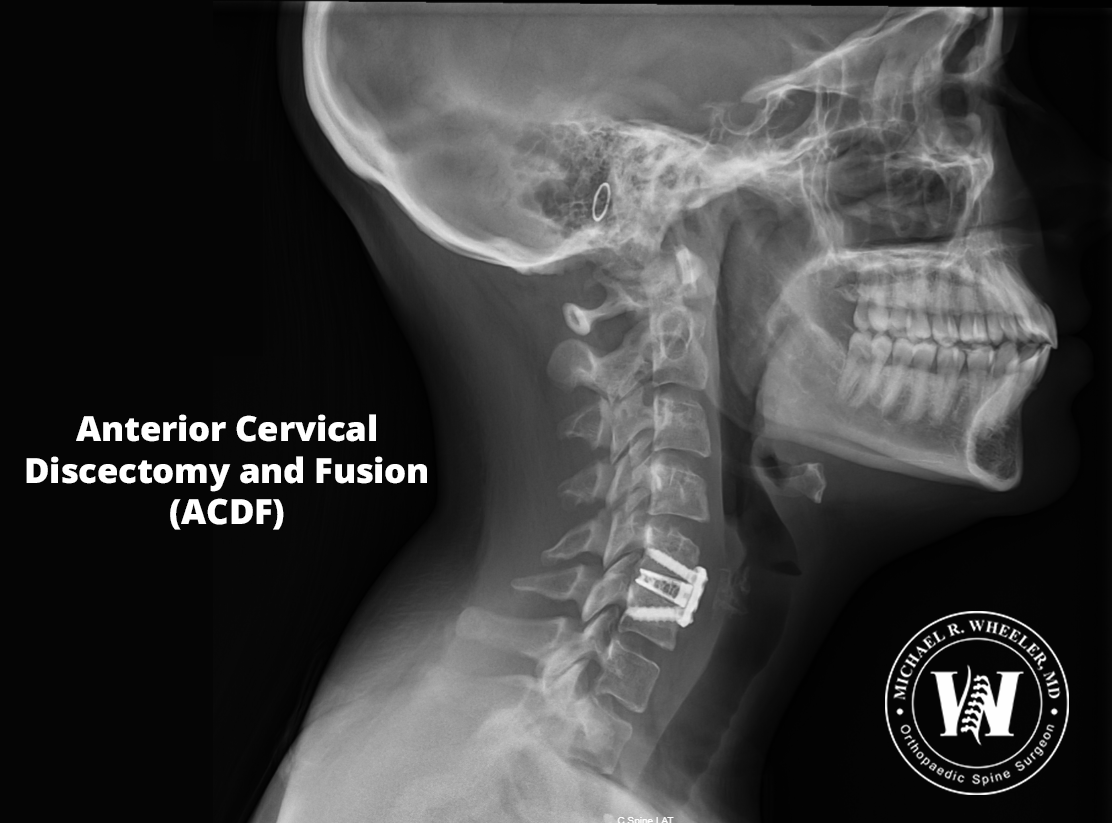
Discs in the cervical spine (or neck) can degenerate over time or herniate, causing pressure on the spinal cord or the exiting nerve roots. This can lead to neck pain and/or pain, weakness, numbness, or tingling of the shoulder, arm, or hand on the affected side. Anterior Cervical Discectomy and Fusion or ACDF is a surgical procedure used to take the pressure off affected nerves by removing the herniated or degenerated disc of the cervical spine. During this procedure, an incision is made in the front of the neck to remove the disc. Depending on the number of problematic discs, one or more discs may be removed. Once the disc(s) is removed, a cage filled with bone graft is inserted into the space to fuse the bones above and below. A small metal plate is usually placed to hold everything in position.
Benefits of Anterior Cervical Discectomy and Fusion (ACDF)
- Relief of arm and shoulder pain caused by pinched nerves in the neck
- Relief of weakness, numbness, or tingling of the arms caused by pinched nerves in the neck
- Relief of neck pain due to degenerative discs in the neck
- Restoration of proper cervical alignment
Patients who would benefit from Anterior Cervical Discectomy and Fusion (ACDF)
- Patients who have neck pain due to degenerative or herniated discs of the neck
- Patients with shoulder/ arm weakness, pain, numbness, or tingling due to pinched nerves of the neck that have failed conservative treatment
Procedure
Positioning: The patient is positioned supine (on his or her back). General anesthesia is used for this surgery.
Neuro monitoring set up: Advanced monitoring of the nerves and spinal cord is used throughout the entire surgery that allows for safe monitoring of each nerve and its function.
Incision: A small incision is made on the front of the neck.
Exposure: The muscles and blood vessels of the neck are carefully moved out of the way to allow access to the spine.
Identifying the affected level: X-ray is used to confirm the appropriate surgical level.
Disc removal: The diseased disc and any bone spurs are removed.
Decompression: Once the disc has been removed, the pressure is taken off the spinal cord and nerves using direct visualization.
Cage trials: Different sized cages (spacers) are trialed in the disc space to ensure the correct size spacer is used for each individual patient.
Placement of the cage: The selected spacer is filled with bone graft and is carefully placed between the vertebrae. X-ray is used to confirm adequate positioning of the cage.
Plate placement: A small metal plate is screwed into place to secure the bones and cage.
Incision closure: The incision is closed with absorbable suture and a dressing is placed.
Risks and complications associated with ACDF
Although risks associated with Anterior Cervical Discectomy and Fusion (ACDF) are rare, patients undergoing this surgery should be aware of the risks involved and discuss the following with the surgeon prior to surgery:
- Hoarseness – this is usually temporary and usually resolves within a few days after surgery
- Trouble swallowing – this is usually temporary and usually resolves within a few days after surgery
- Horner’s Syndrome – this is an extremely rare complication caused by damage to the sympathetic nerves
- Damage to the esophagus
- Damage to the blood vessels of the neck
- Spinal cord or nerve injury
- Pain, bleeding, infection – which are risks of any surgery
Recovery
- Patients usually wake up from surgery with immediate relief of arm or shoulder pain.
- Sometimes, patients may need to wear a collar after surgery for a couple weeks to promote healing.
- Depending on the number of surgical levels, the patient may discharge home the same day of surgery.
- Complete recovery from surgery varies from patient to patient, but patients can usually return to normal activities 6-12 weeks after surgery.
ACDF vs Cervical disc replacement
ACDF is an alternative surgery to cervical disc replacement. Both surgeries are excellent procedures designed to treat similar problems. There are subtle differences that make one surgery preferential over the other depending on the patient’s symptoms, imaging, goals, age, etc. The decision regarding which surgery is best for the individual patient should be discussed with the surgeon.

